Bowel Obstruction Surgery — Treatment for Intestinal Blockage (Emergency/Planned)
Bowel Obstruction Surgery is performed when the small or large intestine becomes blocked and the blockage cannot be safely treated with medications, decompression, or endoscopic methods—or when there are signs of a dangerous complication. Depending on the cause and severity, surgery may be done laparoscopically or through an open approach, and may be urgent or emergency.
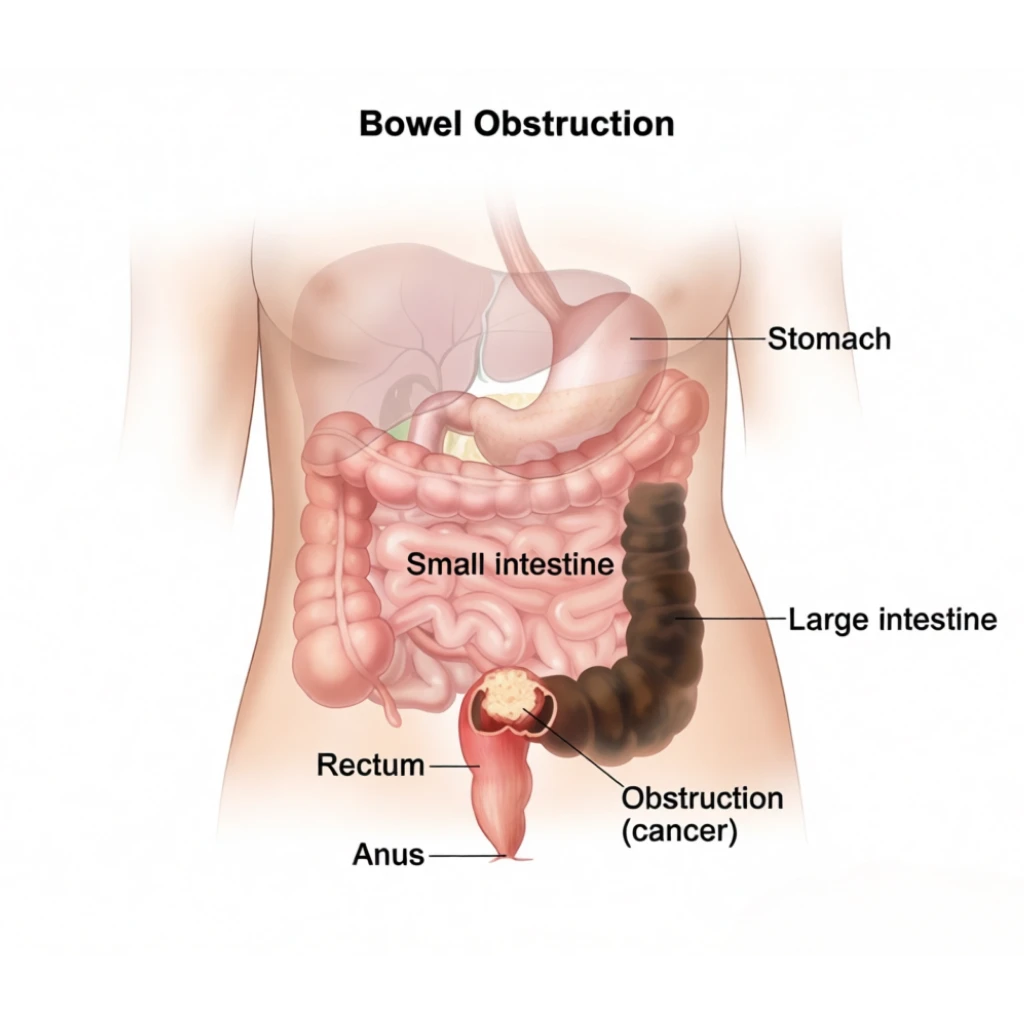
What is a Bowel Obstruction?
A bowel obstruction happens when food, fluids, and gas cannot pass normally through the intestine. It can be:
- Partial or complete
- In the small bowel or large bowel
Common causes include:
- Adhesions (scar tissue) after previous abdominal surgery (very common)
- Hernias
- Tumors (especially in large bowel obstruction)
- Twisting of the bowel (volvulus)
- Inflammation/strictures (e.g., Crohn’s disease)
- Intussusception (more common in children, but can occur in adults)
Warning Signs (Seek Urgent Care)
Get immediate evaluation if you have:
- Severe abdominal pain/cramping
- Persistent vomiting
- Swollen/distended abdomen
- Inability to pass stool or gas
- Fever, fast heartbeat, severe tenderness
These may indicate strangulation, ischemia, or perforation, which are emergencies.

When is Surgery Needed?
Surgery may be required if:
- The obstruction is complete or worsening
- Conservative treatment fails (fluids, NG tube decompression, observation)
- There are signs of bowel strangulation (loss of blood supply) or perforation
- The cause is a condition that requires correction (e.g., hernia, tumor, volvulus)
How is Bowel Obstruction Surgery Done?
The operation depends on the cause and bowel condition. It may involve:
- Adhesiolysis: releasing scar tissue bands causing blockage
- Hernia repair if a hernia is trapping bowel
- Resection: removing a damaged or non-viable bowel segment
- Tumor resection if a mass is obstructing
- Stoma creation (temporary or permanent) in selected cases for safety
Laparoscopic vs Open
- Laparoscopic: smaller cuts, faster recovery in selected stable cases
- Open surgery: preferred when obstruction is severe, bowel is distended, or complications are suspected
The safest approach is chosen based on imaging, severity, and intra-operative findings.
Pre-Operative Evaluation (Typical Workup)
In the emergency setting, assessment may include:
- Physical exam and vital signs
- Blood tests (CBC, electrolytes, kidney function, inflammatory markers)
- CT scan (often the key test to locate the obstruction and detect complications)
- IV fluids and electrolyte correction
- Nasogastric (NG) tube for decompression if needed
- Antibiotics if perforation/ischemia is suspected
Risks & Possible Complications
Potential risks include:
- Infection, bleeding
- Bowel injury or leakage at reconnection site (if resection/anastomosis done)
- Ileus (slow bowel movement after surgery)
- Recurrence, especially with adhesions
- Blood clots (rare but serious)
Your surgeon will explain risks based on your specific operation and health status.
Pre-Operative Evaluation (Typical Workup)
Your surgeon may request:
- Upper endoscopy (gastroscopy) + biopsy
- CT scan of chest/abdomen/pelvis (and/or endoscopic ultrasound in some cases)
- Blood tests (CBC, liver/kidney profile) and nutritional assessment
- Tumor markers or specialized tests depending on tumor type
- Anesthesia and medical fitness evaluation

Recovery & Aftercare
Recovery depends on the cause and whether resection was needed:
- Pain control and early mobilization
- Gradual return of bowel function (passing gas, bowel movements)
- Diet progression from liquids to regular foods
- Monitoring for infection, leakage (if bowel was reconnected), or recurrent obstruction
- Hospital stay varies (often longer if it was an emergency or resection was performed)

Why Choose Us?
With Dr. Ahmed Ali Abdelbary, your treatment is built around:
- Clear evaluation and procedure selection
- Patient-first safety approach
- Structured follow-up and guidance
- Modern bariatric and laparoscopic standards
FAQ ideas:
Some partial obstructions—especially due to adhesions—can improve with fluids and decompression, but surgery is required if there is complete blockage, worsening symptoms, or signs of complications.
Not always, but it can become an emergency quickly. Severe pain, fever, and inability to pass gas/stool are red flags.
Only in certain cases, depending on the bowel condition and safety of reconnection.

Book a Consultation
If you want a professional assessment and guidance on the most suitable option for your condition, book your consultation today.